 Commentary by Travis King, Pharm.D, BCP
Commentary by Travis King, Pharm.D, BCP
By now, I’m certain you’ve all seen the news stories/headlines hinting that the next big viral pandemic is upon us – that virus being the Middle East Respiratory Syndrome Coronavirus (MERS-CoV or MERS).
But before we check to see if the sky is falling, let’s take a brief look at the history of these coronaviruses, and about why the MERS-CoV may not be the greatest threat to Mississippians just yet.
MERS should not be confused with MRSA (methicillin-resistant Staphylococcus aureus) an unfortunately common bacteria associated with both community- and hospital-acquired infections.
The coronaviruses are a quite common group of viruses that have been known to infect animals for decades. The problem with these viruses is their exquisite ability to mutate, allowing them to cross the species barrier. The even more unfortunate aspect of these viruses is that humans are one of those species. The coronaviruses have survived in bats for many years. From bats, they often find their way into small animals (civets, pigs, goats, etc.) that have more intimate contact with bat species than a human. These animals are termed “intermediate hosts” and are often domestic in nature, living in areas with both dense animal and human populations.
After repeated exposure to humans by nature of close animal contact, these viruses mutate, allowing them to multiply in and infect a human host. Once infected, the human may transmit the virus to others via coughs, sneezes, and/or lack of hygiene, much like other viral lung infections. The good news is (was) that in humans, these coronavirus infections were generally limited to the upper airways and presented as the “common cold.” However, about 10 years ago, the world got a glimpse of a coronavirus with a different M.O. – the SARS (Severe Acute Respiratory Syndrome) virus. This particular virus was notable for its ability to cause lower respiratory tract disease, resembling a severe pneumonia. Fortunately, the mortality rate associated with this virus was low (about 10-15 percent), and its human-to-human transmission was quite inefficient. Subsequently, the SARS scare fizzled out quickly.
Eight or so years passed with no real emergence of an atypical coronavirus — until 2012.
In September 2012, a 60-year-old man in Saudi Arabia succumbed to an infection that manifested as lung and kidney failure. About this same time, a 49-year-old patient — this time from Qatar — died in London from a novel respiratory viral infection he acquired while in the Arabian Peninsula. The viral cause was identical in the two patients and represented a variation of a coronavirus not yet encountered until that time.
Over the next year, small outbreaks of infection were noted, the largest of which involved several healthcare workers at a Saudi hospital. These first cases were predominantly found within the Al-Ahsa governate (eastern Saudi Arabia). The emergence and formal recognition of this novel virus prompted the international science community to provide it with a name. That name was “MERS-CoV” or “MERS.”
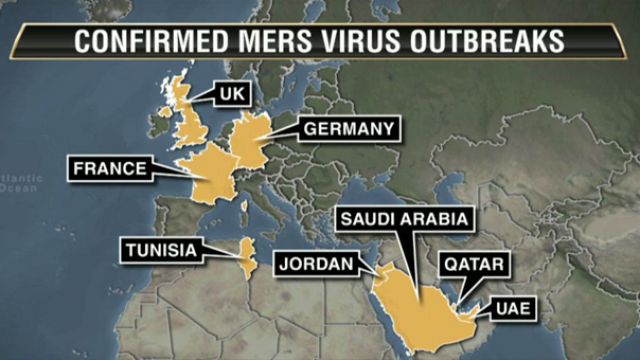
Now fast-forward to May 2014. 400-plus confirmed cases of MERS-CoV have occurred worldwide. The predominance of these infections remain in the Arabian Peninsula (Saudi Arabia, United Arab Emirates, Qatar, Oman, Jordan, and Kuwait. However, an increasing number of infections are occurring in patients with a history of travel to the region and do not “appear” until they return to their home country. The following countries have reported one or more travel-related MERS-CoV infection: the United Kingdom, France, Tunisia, Italy, Malaysia, and now … the United States. The first case seen in the U.S. was found in an individual who lived and worked in Riyadh, Saudi Arabia, and it is highly probable that this is where he contracted MERS-CoV. From Riyadh, he flew to Chicago via London’s Heathrow and then took a bus from Chicago to Indiana, where he is currently being managed and is soon to be released.

So, Where’d It Come From?
From what we can tell, the MERS-CoV originated in a bat species specific to the Middle East. Viral particles have been seen in the Egyptian Cave Bat, but it is not certain at this time if this is the only viral reservoir. As mentioned earlier, it is unlikely that humans have prolonged/repeated exposure to these bat species, so an intermediate host is likely involved. Surprisingly, the MERS-CoV has been circulating in the dromedary camel for some time, and it is suspected that these camels serve as the intermediate host between bats and humans. The dromedary camel lives in close quarters with humans. They are frequently domesticated and used for transportation of people and goods. This close and repeated contact has likely facilitated the ability of the MERS-CoV to infect humans.
How Contagious Is It? Who Gets It? And Is It Deadly?
At the moment, it appears that human-to-human transmission has predominantly occurred from patients to healthcare workers. Transmission within family clusters is low. Current data indicates that patients infected with MERS-CoV are not contagious until they develop respiratory symptoms. This is different than some other respiratory viruses where the patient is contagious during the incubation period (the period following infections but prior to symptom development).
These family members/healthcare workers likely had significant, repeated exposure to the secretions of infected patients. This delay in communicability hints at a low Basic Reproduction Number, or R0(R naught) for the MERS-CoV. The R0 of a pathogen refers to the number of secondary cases that a primary infection is likely to generate; a virus with a R0 greater than 1 is generally more efficiently transmitted than a virus with a R0 less than 1. The currently held R0 for the MERS-CoV is about 0.7. This is marginally less efficient than the R0 of the SARS virus (R0=0.8). It should be noted however, that as time progresses, the MERS-CoV R0 is likely to increase. The most important aspect to consider about the MERS-CoV infections to-date is that most infected patients have had a poor immune system or some other underlying illness. The most common underlying illnesses seen have been diabetes mellitus, kidney disease, or lung disease. The average age of patients thus far is 51 years-old, but this virus is certainly not specific to adults.
Finally, the startling aspect of this particular disease is its case-fatality rate. As of now, approximately 30 percent of all infected patients have ultimately succumbed to the disease. This fatality rate is largely dependent on the number and severity of other underlying illness, though it is still problematic in otherwise healthy patients.
What Do We Not Know Yet?
There are a few points worth noting before we make any solid assumptions about the MERS-CoV outbreak. It still is not clear to what degree this virus exists in the general population. Most of the patients infected to-date have had at least one co-morbid/concomitant disease state; the most common being diabetes mellitus. If the MERS-CoV does exist as asymptomatic or mild infections in otherwise healthy patients, its potential to emerge as a pandemic threat may be lessened.
Similarly, it is not clear yet if a single exposure to the virus is enough to result in fulminant infection. It is possible that repeated exposure is required to facilitate full adaptation to the human host. Interestingly, the receptor that the virus uses for entry into the human varies within certain human populations and may explain the lack of a one-size-fits-all infecting virus.
Should Mississippians Worry?
There is always a healthy amount of worry that should accompany the emergence of any novel infection, be it a virus, bacteria, fungus, parasite, etc. However, this particular virus has not yet shown itself to be a perfect contagion. Currently there are no antiviral medications that have been successfully employed in the treatment of this virus and no vaccine exists, though human antibodies that neutralize the virus have been discovered. While these are all less-than-optimal situations from a global standpoint, for Mississippians, the overwhelming concern can be kept to a minimum. The lowered communicability during the incubation phase of the infection should help keep the rapid spread of MERs-CoV in the U.S.at bay. Concern of a MERS-CoV infection is warranted if you develop fever and respiratory symptoms within 14 days of traveling to the Arabian Peninsula or who have had close contact with someone who has been to the Arabian Peninsula AND currently has respiratory symptoms/fever or is considered a Patient Under Investigation (PUI) by the CDC.
As of May 2014, the CDC has not put any travel advisories on trips to the Middle East. The U.S.’s first patient has been quarantined, treated symptomatically, and is recovering per the latest reports. Close contacts /co-travelers of this patient have been identified and evaluated, and it does not appear that any other infections have resulted from the initial case. The most effective means of controlling the disease, at this time, appear to be isolation measures and quarantine.
So, rest easy Mississippi, the sky isn’t falling….yet.
For More Information Please Visit:
CDC’s MERS-CoV Information Page: Middle East Respiratory Syndrome
CDC’s Travel Recommendations: Travelers’ Health: MERS in the Arabian Peninsula
Information regarding first U.S. MERS-CoV Case: MERS Imported to US
Information from the World Health Organization: WHO MERS-CoV Risk Assessment
S. Travis King, PHARM.D., BCP, is assistant professor, Department of Pharmacy Practice, University of Mississippi School of Pharmacy and a HottyToddy.com contributor. King can be contacted about this story at stking@umc.edu

@ Copyright 2026 by HT Media LLC. All rights reserved. HottyToddy.com is an indepent digital entity not affiliated with the University of Mississippi.